Clavicle Fracture
Medical term: Clavicular Fracture
What Is the Clavicle?
The clavicle — commonly called the collarbone — is a long, slightly S-shaped bone that runs horizontally across the top of your chest, connecting your shoulder blade (scapula) to your breastbone (sternum). You can feel it just under the skin at the base of your neck on either side.
The clavicle acts as a strut that holds your shoulder out and away from your chest, giving your arm its full range of motion. Without it, the weight of your arm would pull your shoulder forward and downward. The clavicle also protects the important blood vessels and nerves that travel from your neck down into your arm.
The clavicle is one of the most commonly broken bones in the body — accounting for roughly 2 to 5 percent of all fractures — partly because it sits directly under the skin with very little protective muscle around it, and partly because it absorbs the full force of a fall or impact on the shoulder.
How Does a Clavicle Fracture Happen?
Most clavicle fractures happen in one of three ways:
- A direct blow to the shoulder — the most common cause — such as a fall onto the side of the shoulder, a tackle in football or rugby, or a motor vehicle collision
- A fall onto an outstretched hand — the force travels up the arm and concentrates at the clavicle
- A direct hit to the bone itself — less common, but can occur in a car accident (from the seatbelt) or a sports collision
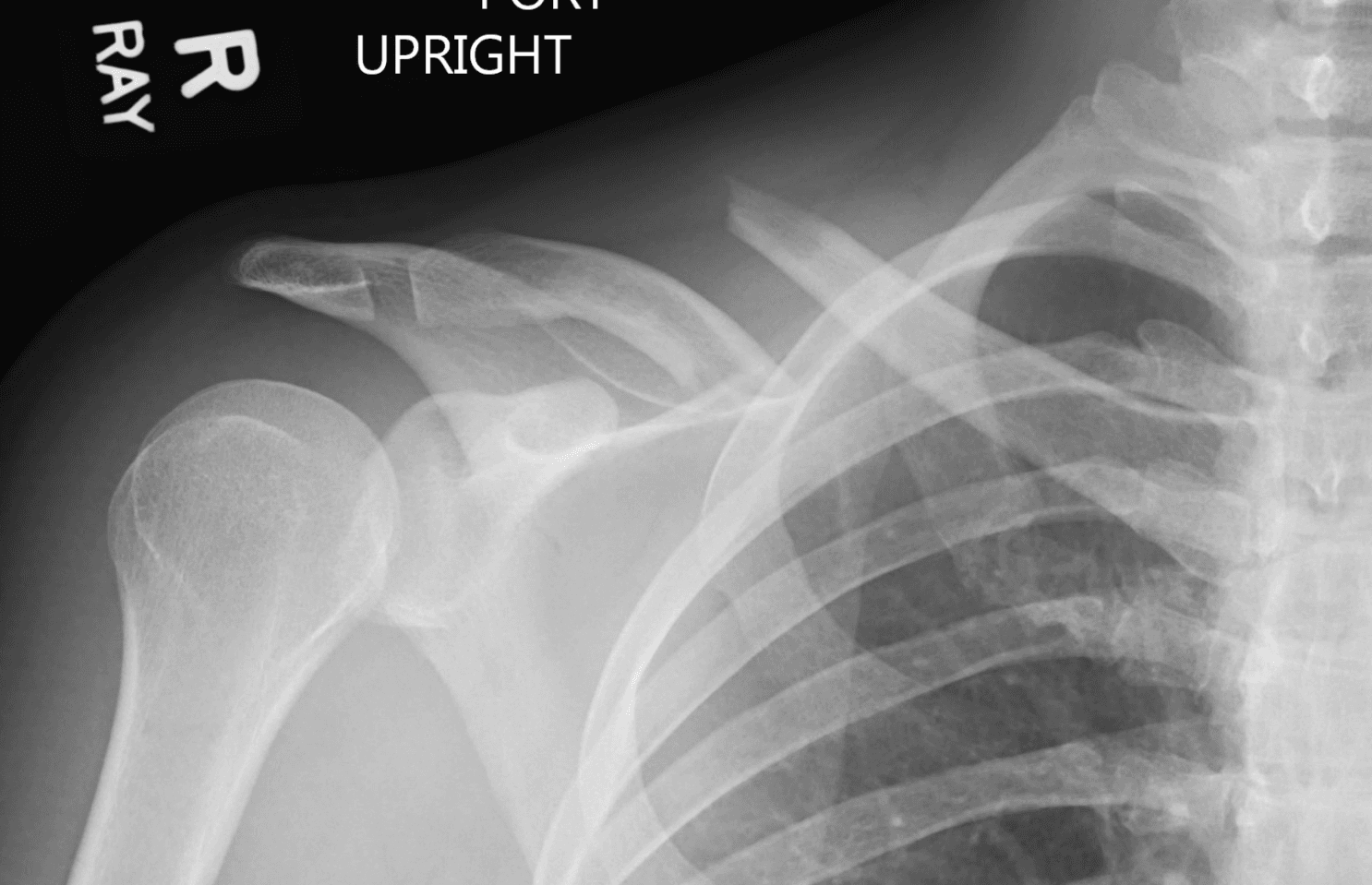
About 80 percent of fractures occur in the middle third (midshaft) of the bone, where it is narrowest and most exposed. Fractures near the shoulder end (lateral third) or near the breastbone (medial third) are less common but often more complex to treat.
Signs, Symptoms, and What to Do First
Signs and Symptoms
- Sharp pain directly over the collarbone, especially with any arm movement
- A visible bump, deformity, or “tent” in the skin over the fracture site
- Swelling or bruising around the shoulder and upper chest
- The injured arm feels heavy; the person tends to hold it close to their body with the other hand
- A grinding or crackling sensation with movement (crepitus)
- In rare cases, numbness or tingling in the arm or hand — seek care promptly if this occurs
When to go to the ER immediately: Seek emergency care if there is an open wound over the fracture, the skin appears to be breaking through, the arm or hand is pale, cold, or numb, or the injury occurred in a high-energy accident such as a car crash or significant fall.
Where to Get Evaluated
- Emergency Room: Go to the ER if the injury was high-energy, if there is an open fracture (bone near or through skin), or if nerve or vascular symptoms are present.
- Urgent Care: Appropriate for an isolated shoulder injury after a minor fall or sports injury in an otherwise healthy adult or child.
- Orthopedic Specialist: If seen first at urgent care or your primary doctor, you will likely be referred to an orthopedic surgeon within a few days for a definitive treatment plan.
How Is It Diagnosed?
- Physical exam — tenderness directly on the bone, visible deformity, limited shoulder movement
- X-rays — the standard first test; typically an AP (front-to-back) view and a 15 to 20 degree cephalic tilt view to assess displacement
- CT scan — ordered when the fracture is near the shoulder joint or breastbone, when surgical planning is needed, or when vascular injury is suspected
- MRI — rarely needed for an acute fracture; may be used if ligament or AC joint injury is suspected
Treatment
Treatment depends on where the fracture is, how much the bone ends are separated, and your overall health, activity level, and goals. The two main paths are non-surgical (closed) treatment and surgical (open) treatment.
Non-Surgical Treatment
Who Is a Candidate?
Most clavicle fractures — roughly 85 percent of midshaft fractures — can be treated without surgery. Non-surgical treatment is generally recommended when:
- The bone ends are not significantly displaced (separated or overlapping less than 1 to 2 cm)
- There is no shortening of the clavicle greater than approximately 2 cm
- The fracture does not involve a joint surface
- There is no nerve or vascular injury
- The patient is medically suitable, including most children, whose bones heal reliably
Immobilization
The goal of immobilization is comfort and protection while the bone heals — it does not hold the bone in perfect alignment the way a cast does for a wrist fracture.
- Simple arm sling — the most widely used method; worn for 2 to 6 weeks depending on comfort and healing
- Figure-of-eight brace — wraps around both shoulders to pull them back; evidence shows it offers no advantage over a sling and is less comfortable for most patients
Most surgeons recommend a standard sling. Your doctor will guide you on when to start gentle movement.
Outcomes
The large majority of non-displaced or minimally displaced fractures heal well without surgery.
- Healing (bony union) occurs in approximately 90 to 95 percent of non-displaced fractures
- Risk of nonunion (failure to heal) increases with greater displacement and shortening
- Patients may notice a visible bump at the healed fracture site — this is a normal callus and usually remodels over 12 to 18 months
Time Off Work — Non-Surgical
| Work Type | Timeframe |
|---|---|
| Desk / light duty | 1 to 2 weeks |
| Moderate physical | 6 to 10 weeks |
| Heavy manual labor or overhead work | 10 to 14 weeks |
Surgical Treatment — Plate Fixation
When Is Surgery Required?
Surgery is clearly required in the following situations:
- Open fracture — bone breaking through the skin
- Neurovascular injury — fracture causing damage to the brachial plexus nerves or subclavian vessels
- Floating shoulder — a combination of clavicle fracture and scapula neck fracture that makes the shoulder completely unstable
- Skin tenting — the bone is pressing against the skin and about to break through
- Polytrauma — patients with multiple injuries who need early mobilization
When Is Surgery Strongly Considered?
Surgery is strongly considered — though not always required — in these situations:
- Significant displacement with shortening greater than 2 cm
- Complete displacement with no bony contact between the two ends
- Athletes or manual workers who need reliable, fast return to full function
- Bilateral clavicle fractures
- Fractures that have failed non-surgical treatment (nonunion or symptomatic malunion)
The Surgical Procedure
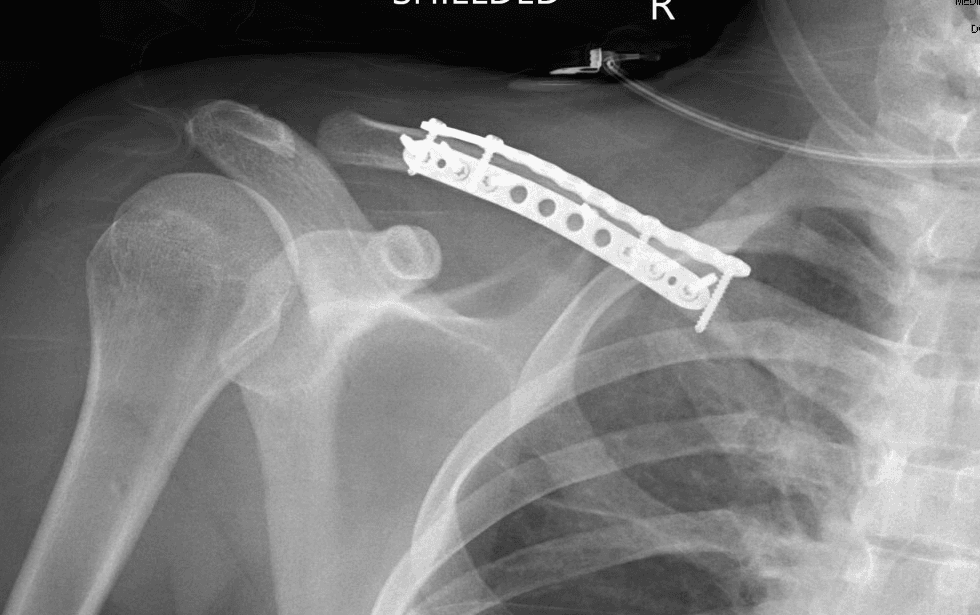
The standard technique is Open Reduction and Internal Fixation (ORIF) using a plate and screws. The surgeon makes an incision directly over the clavicle, realigns the bone fragments under direct vision, and secures them with a low-profile titanium or stainless steel plate fixed with screws. Most cases are performed as outpatient (same-day) surgery under general or regional (nerve block) anesthesia and take approximately 45 to 90 minutes.
Two plating approaches may be used depending on the fracture pattern:
- Superior plating: The plate is placed on top of the clavicle. This is the most common approach, provides strong fixation, and uses widely available implants. The plate may be more prominent under the skin in thin patients.
- Anteroinferior plating: One or two smaller plates are placed on the front and/or undersurface of the bone. This distributes forces differently, may reduce hardware prominence, and is particularly useful for comminuted (multi-fragment) fractures or revision cases.
Potential Complications
- Hardware prominence or irritation — the most common issue; the plate may be felt or seen under the skin, particularly in thin patients (occurs in approximately 10 to 30 percent of cases)
- Hardware removal — approximately 20 to 30 percent of patients eventually request plate removal due to discomfort; usually a minor outpatient procedure after full healing (12+ months)
- Infection — superficial wound infection in 1 to 4 percent; deep infection rare (less than 1 percent)
- Nonunion after ORIF — uncommon (less than 5 percent), particularly in smokers or with inadequate fixation
- Refracture — after plate removal, the bone is temporarily weakened; patients should avoid contact sports for 6 to 8 weeks
- Nerve numbness — the supraclavicular nerves that cross the incision are commonly divided, causing a small patch of skin numbness below the scar; usually permanent but causes minimal functional problems
- Pneumothorax — extremely rare; the lung sits close to the underside of the clavicle
Recovery
Non-Surgical Recovery Timeline
- Weeks 1 to 2: Arm in sling; pain and swelling control with ice and over-the-counter medication. Elbow, wrist, and hand exercises encouraged to prevent stiffness.
- Weeks 2 to 4: Sling use is weaned as comfort improves. Gentle pendulum shoulder exercises begin. Most patients notice significant pain improvement by week 3.
- Weeks 4 to 6: Active shoulder motion introduced as X-rays confirm early healing. Sling typically discontinued.
- Weeks 6 to 12: Progressive strengthening; most patients return to light sports and full daily activities.
- Months 3 to 6: Return to full contact sports and heavy labor once X-rays confirm solid union and strength is symmetric.
Healing timeline varies. Older patients, smokers, and those with more displaced fractures generally take longer.
Surgical Recovery Timeline
- Days 1 to 3: Arm in sling; wound care begins. Pain is typically mild to moderate and well controlled with medication.
- Weeks 1 to 2: Sutures removed; gentle range-of-motion exercises begin under surgeon or physical therapist guidance.
- Weeks 2 to 6: Progressive shoulder motion; sling weaned. The plate provides immediate stability, so motion can usually advance faster than with non-surgical treatment.
- Weeks 6 to 8: X-rays confirm healing; light strengthening begins.
- Months 2 to 4: Return to most work and recreational activities.
- Month 6+: Full return to contact sports and heavy manual work once cleared by surgeon.
Return to Work Comparison
| Work Type | Non-Surgical | Surgical |
|---|---|---|
| Sedentary / desk work | 1 to 2 weeks | 1 to 2 weeks |
| Light physical / retail | 4 to 6 weeks | 3 to 5 weeks |
| Moderate physical | 8 to 12 weeks | 6 to 10 weeks |
| Heavy manual / overhead | 12 to 16 weeks | 10 to 14 weeks |
Long-Term Outcomes
For significantly displaced midshaft fractures, the medical literature generally supports the following:
- Nonunion occurs in approximately 15 percent of completely displaced fractures treated non-surgically, versus 2 to 3 percent after ORIF
- Malunion is more common with non-surgical treatment, but most patients are not significantly limited by mild shortening
- Functional outcomes — randomized controlled trials found ORIF resulted in faster return to function and lower nonunion rates for displaced fractures, but comparable long-term outcomes at 1 to 2 years
- Patient satisfaction is similar between operative and non-operative groups at final follow-up in most studies
- Re-operation is higher in the surgical group due to plate removal; the non-surgical group has re-operations for nonunion repair
Each patient is different. Your surgeon will weigh fracture characteristics, activity level, occupation, and overall health to recommend the best treatment for you.
Physical Therapy
Rehabilitation is an important part of recovery — whether or not surgery was performed. Physical therapy restores shoulder range of motion, strength, and function, and reduces the risk of long-term stiffness.